




Drug Delivery
Latest News
Advertisement
Latest Videos



Advertisement
More News
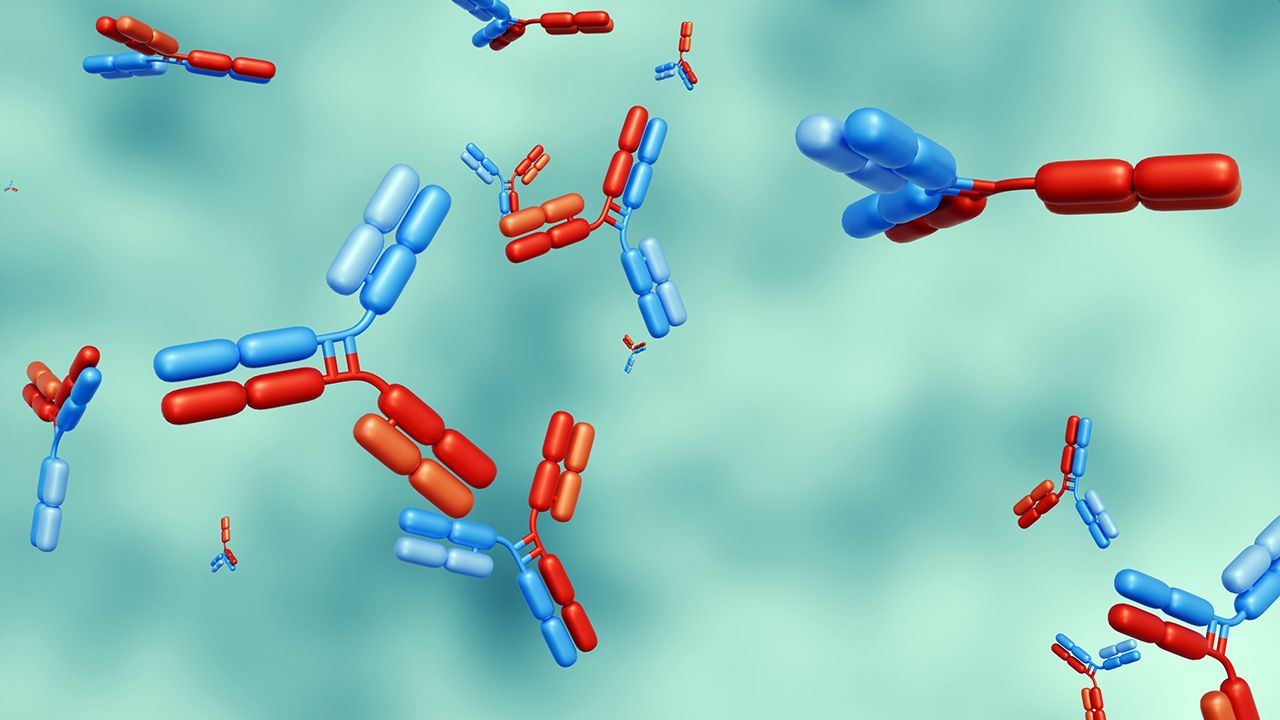
FDA’s breakthrough therapy designation for Johnson & Johnson’s co-formulated bispecific antibody therapy validates dual EGFR/MET targeting in HPV-negative head and neck cancer.

PharmaResearch’s DOT-based nanoparticle platform enters US clinical testing, highlighting delivery innovation aimed at improving tolerability in solid tumor therapies.

NeoVac first-in-human data suggest that optimized lipid nanoparticles may improve mRNA tolerability, enabling repeat dosing and broader therapeutic use.

Study data show high-dose nusinersen can improve function and slow neurodegeneration, informing future SMA dosing strategies and lifecycle management.

The guidance provides clarity to drug manufacturers on offering lower drug prices directly to patients, including patients on Medicare and Medicaid.

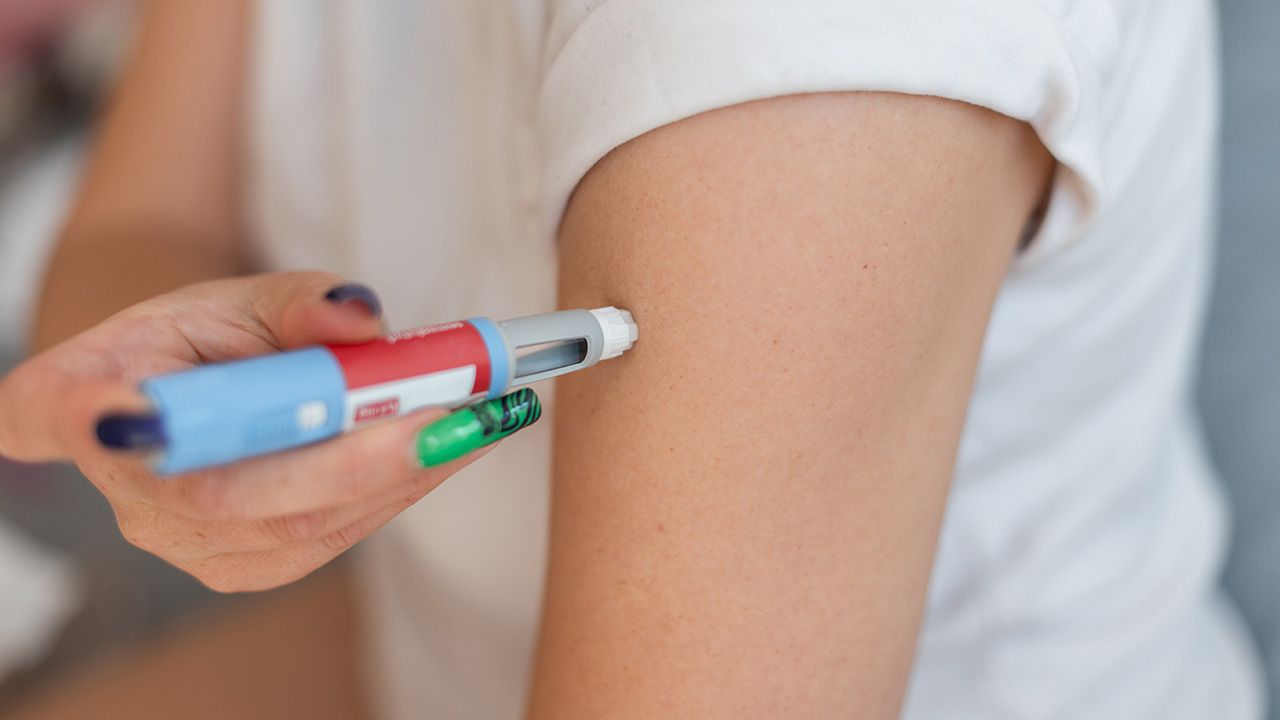
European regulators authorize AstraZeneca’s anifrolumab pen for lupus, reinforcing industry momentum toward self-injected biologics and decentralized immunology care.
Surface modification with targeting ligands increases the advantages offered by nanoscale delivery.

The transformative impact of complex biopharmaceuticals hinges on integrating advanced delivery systems, often accelerated by AI modeling, with robust manufacturing practices and regulatory alignment to ensure stability, safety, and effective patient access.

The company demonstrates advances in glioma hydrogel, high-concentration biologics, and nanoencorafenib licensing, impacting drug delivery strategies.

The spray-dried formulations for Ethris’ mRNA vaccine candidates will be developed at Lonza’s Bend, Ore., Center of Excellence in accordance with GMP standards.

The 2025 Pharmapack Awards recognize both commercial products and innovations that are shaping the future of pharmaceutical packaging.
Lonza will develop spray-dried formulations for an intranasally delivered biologic using a reformulated biologic drug candidate for obesity in Iconovo’s pipeline.
The transaction, which was first announced in September 2024, expands Phillips Medisize’s inhalation drug delivery capabilities.
The companies will develop a platform that can enable rapid development of DPI products.
EXO Biologics and its subsidiary, ExoXpert, have received GMP certification of a European exosomes manufacturing facility and have successfully loaded mRNA and DNA payloads into GMP-grade exosomes for drug delivery.
Lonza’s new tailored offering leverages the company’s bi-layer capsule manufacturing technology.
Under the collaboration, the companies will create and test circVec DNA–LNP formulations with an eye toward potential therapeutic applications.

The collaboration aims to develop precision genetic medicines using ViaNautis’ proprietary polyNaut technology platform.

This podcast explores the challenges of and the progress made so far by the biopharma industry toward alternative drug delivering methods for biologic drugs.

Alternative delivery methods for biologics continues to be explored that offer less invasive, less painful administration.

AAV and lentivirus both have pros and cons in their use for specific gene therapy applications.
The company is referring to its search for innovative approaches as crowdsourcing and will award at least one cash prize.

At BIO 2024 in San Diego, John Dunlop, PhD, chief scientific officer at Aliada Therapeutics, sat down for an interview with BioPharm International to discuss the firm’s MODEL platform and its potential impact on therapeutic delivery for brain-related conditions.
Swiss CDMO CordenPharma and Spain-based Certest will collaborate on the development of ionizable lipids for LNP formulations.
The 2024 Pharmapack Europe Award winners include companies involved in ground-breaking innovations in novel drug delivery solutions, reusable connected devices, and recyclable packaging.
Advertisement
Advertisement